

Head and Neck Cancer Surgery

The most complex, compact, and critical region of human anatomy in terms of vital functions is the head and neck area. In addition to fundamental functions that connect us to life, such as breathing, speaking, swallowing, smelling, and tasting, our facial expression and outward appearance are also shaped by the flawless architecture of this region. Head and neck cancers are malignant tumoral formations that arise in a wide area starting from the lips and including the oral cavity (tongue, palate, gums), pharynx, larynx (voice box), salivary glands, paranasal sinuses, and thyroid gland.
In the past, when “cancer surgery” was mentioned, the first thing that came to mind was simply aggressive removal of the tumor from the body. However, our philosophy in modern head and neck surgery has completely changed. In the surgical approaches we apply today, our primary goal is to save the patient’s life by clearing the tumor leaving zero residue behind (with negative surgical margins); our secondary and equally important goal is to preserve organ functions (voice, swallowing) and the patient’s aesthetic appearance to the maximum extent. Thanks to revolutionary advances in microsurgical methods, laser technologies, and reconstructive surgery, a head and neck cancer diagnosis is no longer an irreversible loss, but a disease that can be overcome with proper and multidisciplinary treatment.
What Causes Head and Neck Cancers and What Are the Symptoms?
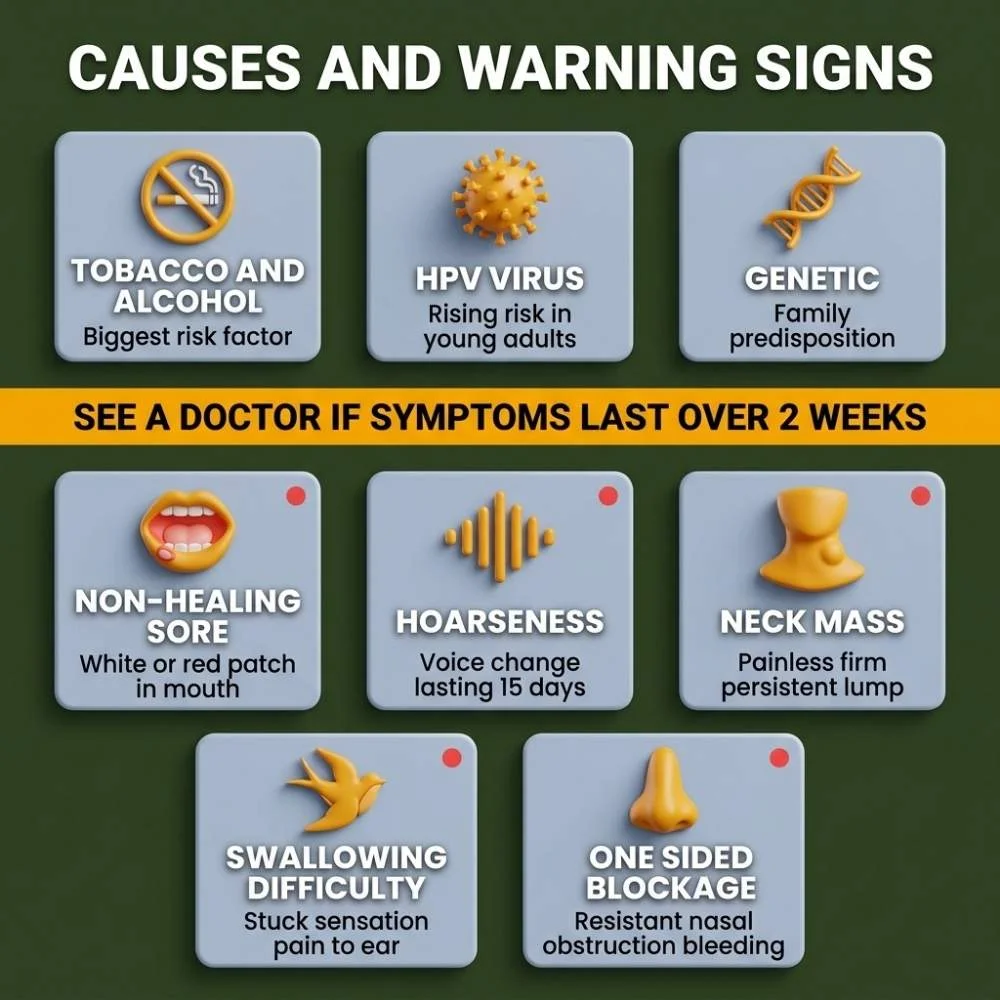
Historically, the two biggest culprits in the development of cancers in this region have been tobacco products (cigarettes, pipes, cigars) and excessive alcohol consumption. The combined use of both exponentially increases the cancer risk. However, in recent years, there has been a significant increase in tonsil and base of tongue cancers, especially in young adults who have never smoked; the main reason for this is HPV (Human Papilloma Virus) infection.
Head and neck cancers usually give warning signs in the early stages. If any of the following symptoms last longer than 2 weeks, a detailed ENT and Head & Neck Surgery examination is strictly required without wasting time:
- Non-Healing Sores in the Mouth: White/red patches and ulcers on the tongue, gums, or cheek mucosa that are prone to bleeding, painful, or painless.
- Hoarseness and Voice Changes: This is the earliest and most prominent harbinger, especially of laryngeal (voice box) cancer. Hoarseness lasting longer than 15 days must be examined endoscopically.
- Swelling in the Neck (Mass): Hard lumps that do not go down for weeks, are generally painless, and progressively enlarge, which can be a sign of spread (metastasis) to the neck lymph nodes.
- Difficulty Swallowing (Dysphagia): A feeling of food getting stuck, severe pain radiating to the ear when swallowing, or liquids escaping into the nasal passage.
- Unilateral Nasal Congestion or Bleeding: Unilateral, persistent symptoms especially seen in sinus and nasopharyngeal cancers.
Modern Surgical Methods in Head and Neck Cancers
Cancer surgery is a tailor-made process; the location, stage, and biology of every patient’s tumor are different. In our clinic, the most up-to-date surgical techniques adhering to world standards, which focus on preserving the patient’s quality of life, are applied:
1. Minimally Invasive Transoral (Through the Mouth) Surgery
This is a closed surgical method applied especially in early-stage larynx (vocal cord), tonsil, and base of tongue tumors by entering entirely through the oral cavity without making any external incision on the neck.
- Transoral Laser Microsurgery (TOLM): It is the process of millimetrically vaporizing or cutting out the tumor using a high-precision carbon dioxide (CO2) laser under a microscope. Healthy tissue is preserved to the maximum extent, and the patient is usually discharged in a short time, often without the need for a tracheostomy (creating a hole in the windpipe).
2. Neck Dissection (Removal of Lymph Nodes)
By their nature, head and neck cancers tend to spread (metastasize) first to the lymph nodes in the neck. Neck dissection is the procedure of removing not only the tumorous organ but also the at-risk or diseased lymph nodes in the neck as a single block. In modern surgery, the procedure is performed while meticulously preserving the carotid artery, the vagus nerve, and the nerves that control shoulder movements (Functional Neck Dissection).
3. Advanced Stage Tumor Surgery and Reconstruction
In cases where the tumor is at an advanced stage, a large portion of the jawbone, tongue, or a section of the pharynx may need to be removed. This is where the power of modern surgery comes into play. Instead of the removed tissue, tissues taken from another part of the body (leg bone, arm skin, or back muscle), along with their hair-thin blood vessels, are transferred by being sutured to the vessels in the neck under a microscope (Microvascular Free Flap Surgery). Thanks to this “Reconstruction” process, a new tongue can be made for the patient with tissue taken from the arm, or a new jaw with bone taken from the leg. Thus, the patient can eat through the mouth again, speak, and no severe disfigurement occurs on the face after the treatment.
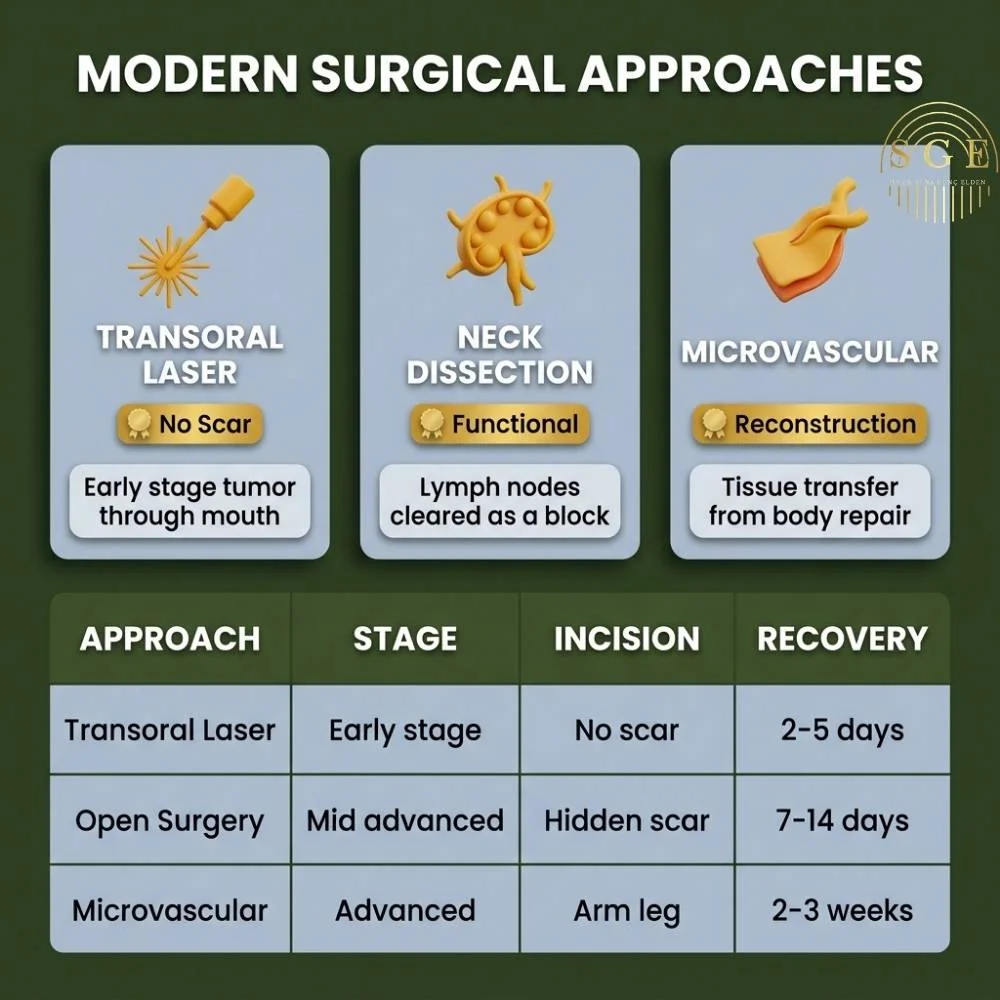
Comparative Table: Head and Neck Cancer Surgery Approaches
| Surgical Approach | Best Suited For | External Incision / Scar | Function Preservation (Voice/Swallowing) | Recovery Time |
| Transoral Laser (Closed) | Early-stage larynx and oral cavity cancers | No external scar (Only inside the mouth) | Very High (Organ is fully preserved in early stages) | Very Fast (2-5 Days) |
| Open Surgery + Neck Dissection | Mid/Advanced stage tumors, spread to neck lymph nodes | Incision hidden in skin creases on the neck | Moderate – High (Depends on tumor size) | Standard (7-14 Days) |
| Microvascular Reconstruction (Free Flap) | Very advanced cases where jaw, wide tongue, or pharynx tissue is removed | Incision on face/neck and donor site (arm/leg) | Function and aesthetics restored via tissue transfer | Long (2-3 Weeks hospital stay) |
Step-by-Step Treatment and Recovery Process
Head and neck cancer surgery is not just an operation; it is an organized team effort.
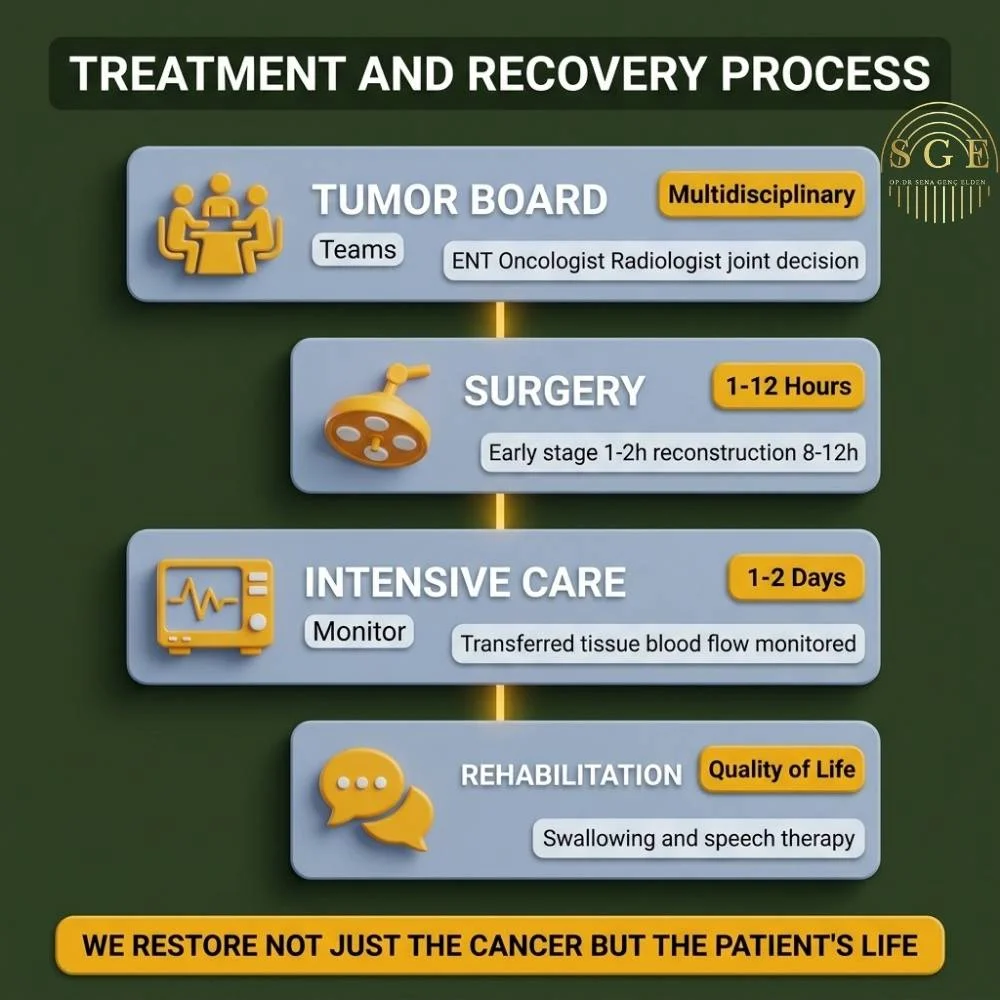
1. Tumor Board (Multidisciplinary Approach): This is the most critical stage in our clinic. The patient’s pathology results, PET-CT, and MRI scans are jointly evaluated by the “Tumor Board,” consisting of an ENT Surgeon, Medical Oncologist, Radiation Oncologist, and Radiologist. Whether surgery, radiotherapy, or a combination of both will yield the best result is determined according to international protocols.
2. Operation Phase: The planned surgery is performed under general anesthesia. While an early-stage laser surgery takes 1-2 hours, a comprehensive surgery involving neck dissection and microsurgical tissue transfer (free flap) can take between 8 to 12 hours.
3. Intensive Care and Hospital Monitoring: Patients undergoing major reconstruction surgery are generally hosted in the Intensive Care Unit for the first 1-2 days to closely monitor the blood flow (vitality) of the transplanted tissue. They are then transferred to a regular ward.
4. Rehabilitation (Speech and Swallowing Therapy): In organ-preserving surgeries (such as tongue or larynx) or in patients undergoing tissue transfer, postoperative rehabilitation is of vital importance. Shortly after surgery, our patients undergo swallowing reflex recovery and voice/speech exercises accompanied by expert therapists. Our goal is not only to clear the cancer but to return the patient to social life in the best possible way.
Frequently Asked Questions (FAQ)
You can quickly access answers to the most common questions and find detailed information about the treatment process here.
Will I completely lose my voice if I have laryngeal cancer surgery?
Thanks to laser surgery or partial laryngectomy techniques applied in laryngeal cancers diagnosed in the early stages, the patient’s voice is largely preserved (even if it is a bit deeper or hoarse), and the patient continues to speak normally. Only in very advanced-stage tumors might the entire voice box need to be removed (Total Laryngectomy). However, even in this case, thanks to “voice prostheses” placed in the windpipe, our patients can learn to speak quite understandably and fluently a few weeks after surgery. The voice is never completely lost; only the method of production changes.
Will a hole be made in my throat after surgery? Is this a permanent condition?
After major surgeries in the head and neck region, a temporary hole (Tracheostomy) is opened in the windpipe to secure the airway and prevent post-operative tissue swelling (edema) from blocking the patient’s breathing. This is a safety measure. As the swelling in the surgical area subsides and the patient begins to breathe normally (usually within 5-10 days), this hole is closed and heals on its own. Only in total laryngectomy cases, where the entire voice box is removed, is the tracheostomy (hole in the throat) permanent.
Will I have very large scars or disfigurement on my face or neck after cancer surgery?
Aesthetic concerns are at the forefront of modern surgery. Incisions for neck dissection are planned to be hidden within the natural skin lines or creases of the neck (apron incision); when healed, they remain as a fine line from the outside. In cases where the jaw, nose, or a part of the face is removed, facial symmetry and anatomical shape are rebuilt as close to perfect as possible using microvascular reconstruction (tissue transfer) and 3D-printed implants.
Will I need to receive radiotherapy or chemotherapy after surgery?
This situation depends entirely on the pathological examination of the tumor and lymph nodes removed during surgery. If the tumor is at a very early stage, its margins are clear, and it has not spread to the lymph nodes, additional treatment is generally not required. However, if the tumor margins are close, it has an aggressive (fast-growing) structure, or metastasis is detected in the lymph nodes, radiotherapy (radiation treatment) is planned about 1 month after the surgery to insure the success of the surgery and eliminate the risk of recurrence.
Will I be able to eat after oral cancer surgery?
Yes. In comprehensive surgeries where reconstruction is performed with external tissue transfer, the patient is fed with a thin tube (nasogastric tube) extending from the nose to the stomach for the first 10-15 days so the new tissues can heal. When healing is complete, the tubes are removed, and accompanied by a swallowing therapist, a transition is made first to liquid, then pureed, and finally solid foods, returning to normal nutrition.

Op. Dr. Sena Genç Elden
Otolaryngologist (ENT Specialist)
Op. Dr. Sena Genç Elden, following her medical and residency training, completed Facial Plastic Surgery School and gained experience as a chief physician; she possesses national and international clinical expertise alongside world-renowned surgeons and currently continues her practice at her own private clinic in Serdivan, Sakarya.
Take the First Step for a New Beginning!
Address:
Contact Us
Mail: info@drsenagencelden.com
Let’s Fight Cancer Together, Preserve Your Life and Functions
Suspecting or receiving a cancer diagnosis in your head and neck region can be one of the toughest moments in your life. We deeply understand the anxiety you and your family feel, and the fear of losing your voice, not being able to eat as before, or your outward appearance changing. However, with microsurgery and reconstruction techniques—the pinnacle of medical science—it is now possible to remove the cancer from your body while ensuring you continue your social life with the same quality. Above all, to hold on to life, your loved ones, and your smile in the mirror; contact us to make the right diagnosis, plan your treatment in our tumor board, and take safe surgical steps together. Your battle is our area of expertise.
References and Scientific Basis
It is an uncompromising principle of our clinic that our patients have transparent access to the most accurate, up-to-date, and scientific information on vital issues. The diagnosis, treatment, and surgical approaches on this page have been compiled with reference to the guidelines of organizations accepted as authorities in oncology and ENT worldwide:
International Clinical Guidelines;
National Cancer Institute (NCI): Head and Neck Cancers – Treatment Options and Reconstruction.
Mayo Clinic: Head and Neck Cancer – Diagnosis and Surgery.
American Head and Neck Society (AHNS): Patient Information on Surgical Resection and Microvascular Reconstruction.
Academic Publications (Surgeon Dr. Sena Genç Elden) ;
- Elden, S. G., et al. (2024). Diagnostic Value of the Video Head Impulse Test in Patients with Vertigo: Can It Be Used as a Screening Tool? ResearchGate
- Elden, S. G., & Güven, E. M. The Effect of Hypericum Perforatum L. (St. John’s Wort) on Prevention of Myringosclerosis After Myringotomy. ResearchGate
- Genç Elden, S., & Demir, D. Investigation of diclofenac sodium’s ototoxic and neurotoxic effects on the rat model. ResearchGate